Notable Cases by Dr. Habib Moshref Razavi:
Todays case: A 65-year-old female with hypertension and hyperlipidemia presented to the ED with a 1-week history of shortness of breath and a 4-week history of dry cough. Her WBC was 16.3, with lymphocytes at 12.9. Hematology service recommended admission for an expedited workup of a lymphoproliferative disorder. Her medical history included a family history of lymphoma and cancer. Despite no exertional chest pain, she experienced significant fatigue and night sweats.
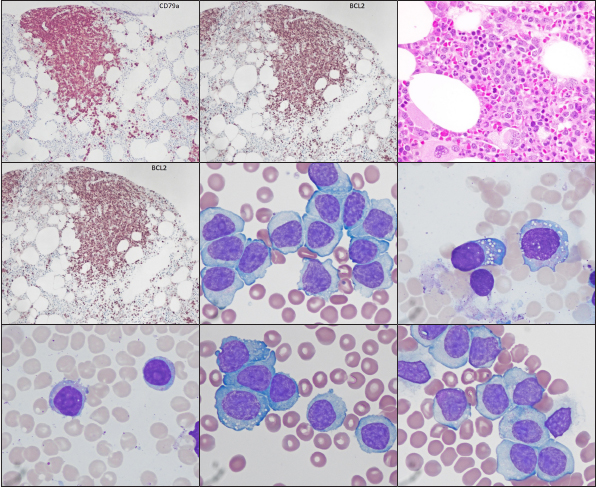
Initial tests revealed splenomegaly (20.6 cm in maximum dimensions in the coronal plane). The patient was admitted for further evaluation, including flow cytometry to determine the underlying cause of her symptoms. A bone marrow biopsy showed normocellular marrow (40%) with an atypical lymphoid infiltrate in a nodular and partially intrasinusoidal pattern. The infiltrate consists of medium to occasionally larger lymphocytes with irregular nuclear contours and prominent nucleoli. Immunohistochemical stains indicated that these atypical lymphocytes are CD20+, Cyclin D1+, and kappa light chain restricted. Flow cytometry confirmed a significant abnormal B-cell population. Cytogenetics reveals a complex karyotype with a MYC rearrangement, but no CCND1/IGH, IGH/BCL2, or BCL6 rearrangements. The findings suggested peripheral blood and bone marrow involvement by splenic B-cell lymphoma with prominent nucleoli (SBLPN), also known as hairy cell leukemia variant (HCL-v), without evidence of transformation to large B-cell lymphoma. (albumin slide of peripheral blood; May-Grünwald Giemsa stain, panels 1-4 X100; panels 6-7 aspirate slide x100 magnification.) View larger images on LinkedIn